Supreme Court-Appointed National Task Force (NTF) on Student Mental Health and Suicides

- 18 Jun 2026
In News:
The Supreme Court-appointed National Task Force (NTF) has submitted its interim report on student mental health and suicides, observing that student suicides are not merely individual mental health issues but reflect structural and institutional failures. The report calls for comprehensive reforms in higher educational institutions to address systemic causes of student distress.
About the National Task Force (NTF)
The National Task Force (NTF) was constituted by the Supreme Court in Amit Kumar & Ors. v. Union of India (2026) under the chairmanship of Justice S. Ravindra Bhat (Retd.), former Judge of the Supreme Court.
The Task Force was mandated to examine the causes of student suicides in higher educational institutions and recommend measures to strengthen institutional support systems and student well-being.
Key Findings of the Interim Report
The NTF concluded that student suicides are the outcome of multiple structural, social, academic, institutional and economic factors, rather than being solely attributable to mental health disorders.
Major findings include:
- Absence of a dedicated legal framework for suicide prevention in higher educational institutions, with existing measures largely limited to non-binding guidelines.
- Over 70% of institutions lack full-time mental health professionals, while less than 4% have structured suicide-risk management systems.
- Social exclusion and discrimination, particularly among SC, ST and OBC students, contribute to higher dropout rates and psychological distress.
- Significant mismatch between the diversity of the student population and faculty representation adversely affects inclusion and academic integration.
- Financial hardship, institutional discrimination and inadequate support mechanisms further increase student vulnerability.
Key Recommendations
The NTF has recommended a systemic approach centred on institutional accountability and student welfare.
Key recommendations include:
- Filling all faculty vacancies, including reserved-category posts, within three months, while ensuring that key administrative positions remain vacant for no more than one month.
- Making mandatory reporting of every student suicide by educational institutions to regulators and State nodal authorities, irrespective of where the death occurs.
- Ensuring 24×7 access to qualified medical and mental health professionals in all residential educational institutions.
- Directing the National Crime Records Bureau (NCRB) to maintain separate data on school and higher education student suicides to facilitate evidence-based policymaking.
Significance
The report shifts the discourse from viewing student suicides solely as individual mental health failures to recognising them as a governance, equity and institutional responsibility issue. Its recommendations aim to strengthen mental healthcare, improve inclusivity, enhance institutional accountability, and support vulnerable student groups. If implemented effectively, the recommendations could contribute significantly to creating safer, more equitable and supportive educational environments.
The Missing Link in India’s Health Strategy: Reimagining Paternal Preconception Care

- 09 May 2026
In News:
For over three decades, India’s RMNCH A (Reproductive, Maternal, Newborn, Child, and Adolescent Health) strategy has been the cornerstone of public health, successfully driving down maternal and neonatal mortality. However, as the focus shifts from mere survival to the biological quality of survival, a critical gap has emerged: the near-total exclusion of fathers from the reproductive narrative.
Emerging science suggests that the "health transmission" to the next generation is a bi-parental process, where a father’s lifestyle and environment long before conception are just as vital as maternal care.
The Crisis of Male Reproductive Health in India
Recent data from 2026 highlights a silent emergency in male fertility and reproductive robustness:
- Declining Sperm Quality: National studies indicate that average sperm counts in Indian men have plummeted from 60 million/ml to 20 million/ml over the last 30 years. Today, only about 25% of Indian men meet normal semen parameters.
- Rising Infertility: Male factors now account for 30%–40% of infertility cases in urban hubs like Kolkata and Pune, largely driven by stress and metabolic syndrome.
- The "Vulnerability" Gap: While more children are surviving birth, many exhibit increased vulnerability to infections and metabolic disturbances—a trend scientists increasingly link to paternal health.
Scientific Evolution: Beyond the "Genetic Passivity" Myth
For a century, the medical community was guided by the Weismann Barrier theory, which argued that somatic (body) cells could not transmit environmental information to germ (sperm/egg) cells. The father was viewed merely as a passive donor of DNA.
However, the discovery of Epigenetics has overturned this model:
- Sperm as a Messenger: Sperm contributes a complex cargo beyond DNA, including microRNAs (small non-coding RNAs). These act as molecular messengers of the father's environment.
- The Exercise Impact: A landmark 2026 study in Cell Metabolism demonstrated that exercise in male mice altered sperm microRNAs, which then programmed embryos for enhanced metabolism and endurance. Offspring of active fathers showed a 30%–40% increase in running distance and better oxygen consumption ($VO_2$).
- Environmental Programming: Factors like smoking, obesity, alcohol, and stress "re-programme" the embryo’s gene expression during a critical window immediately after fertilization, before the embryo begins its own gene expression.
Barriers to Paternal Inclusion
Despite this scientific shift, several factors keep fathers "missing" from Indian health interventions:
- Maternal-Centric Policy: National programs focus almost exclusively on Antenatal Care (ANC) and institutional deliveries, positioning men as financial providers rather than biological participants.
- The Stigma of Infertility: Social taboos place the entire burden of fertility on women. Men represent only a fraction of patients at fertility clinics, leading to "silent grief" and under-diagnosis.
- Lack of Preconception Awareness: Most men seek medical help only after years of trying to conceive, by which time paternal age and poor lifestyle choices may have already degraded sperm quality.
- Systemic Invisibility: Clinical settings for maternal care are often women-only spaces, making men feel unwelcome or irrelevant to the biological process.
Challenges in Implementation
- Slow Lifestyle Changes: Improving sperm health requires 3–6 months of consistent diet and exercise—a "hard sell" compared to quick-fix medical technologies.
- Environmental Toxins: Exposure to endocrine disruptors (plastics, pesticides) is rising faster than our ability to screen prospective fathers.
- Fragmented Data: Much of the evidence on paternal programming currently relies on animal models, leading to policy hesitancy in applying these findings to human clinical guidelines.
Way Forward: A Bi-Parental Framework
To ensure the health of future generations, India must pivot toward an inclusive health model:
- Paternal Preconception Package: Update the RMNCH A strategy to include lifestyle, diet, and stress screening for men.
- Mandatory Lifestyle Assessments: Integrate risk assessments for men at the time of marriage registration or initial fertility consultations.
- Grassroots Counseling: Train ASHA workers to counsel both parents on how environmental exposures (like smoking) affect child robustness.
- Advanced Diagnostics: Utilize AI-powered semen analysis and home-based testing kits to make monitoring private and accessible.
- National Awareness Campaigns: Launch initiatives like "Healthy Father, Healthy Future" to de-stigmatize male infertility and explain the science of epigenetics.
Conclusion
Fathers are the "missing link" in India’s reproductive health story. Moving beyond the supplementation of iron tablets for adolescent boys, the government must recognize that a father’s health is a low-cost, high-impact lever for improving population health. True reproductive health is not a female responsibility, but a bi-parental mission to ensure the biological robustness of the next generation.
Maternal Health in India: Bridging the Gap from Policy to Outcomes
- 01 Apr 2026
In News:
While India has achieved monumental success in reducing its Maternal Mortality Ratio (MMR), recent global studies highlight that the journey toward the 2030 Sustainable Development Goals (SDG) remains fraught with regional disparities and structural bottlenecks.
The Global and National Landscape: Recent Findings
A 2024 study published in The Lancet provides a sobering look at the current state of maternal mortality. Despite decades of rapid decline, the pace of progress globally has plateaued since 2015.
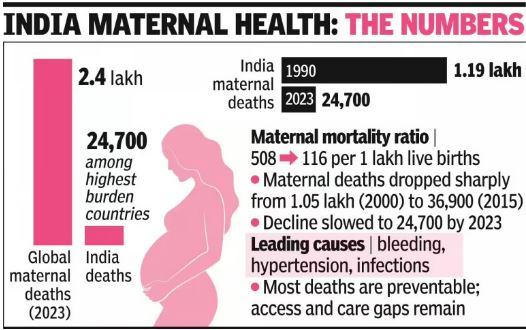
- The Global Burden: In 2023, approximately 2.4 lakh women died due to pregnancy or childbirth-related complications.
- India’s Position: India accounted for 24,700 of these deaths, roughly 1 in every 10 global maternal deaths. This places India among the high-burden nations alongside Nigeria, Pakistan, and Ethiopia.
- Causes of Mortality: Most deaths remain driven by preventable factors, including hemorrhage (excessive bleeding), hypertensive disorders (eclampsia), infections, and complications from pre-existing conditions.
Defining Maternal Mortality: Key Metrics
For administrative and policy purposes, India uses specific terminologies tracked under the Sample Registration System (SRS):
- Maternal Death: The death of a woman during pregnancy or within 42 days of termination, due to causes related to or aggravated by pregnancy, excluding accidental causes.
- Maternal Mortality Ratio (MMR): Number of maternal deaths per 1,00,000 live births.
- Maternal Mortality Rate: Number of maternal deaths per 1,00,000 women in the reproductive age group (15-49).
- Global Target (SDG 3.1): To reduce the global MMR to less than 70 per 1,00,000 live births by 2030.
India’s Progress: Successes and Regional Divergence
According to the National Family Health Survey-5 (2019-21), India has shown remarkable resilience in improving maternal outcomes.
Key Statistical Achievements
- MMR Decline: India’s MMR dropped from 130 (2014-16) to 97 (2018-20), successfully meeting the National Health Policy target of staying below 100 by 2020.
- Institutional Deliveries: A massive leap from 79% (2015-16) to 89% (2019-21). States like Kerala, Tamil Nadu, and Goa have achieved 100% institutional births.
- Rural-Urban Convergence: Even in rural pockets, institutional deliveries have reached 87%, significantly closing the gap with urban areas (94%).
The "Two Indias" Phenomenon
Progress remains highly uneven. While Southern states are nearing or have surpassed the SDG target of 70, states in the "BIMARU" belt, Uttar Pradesh, Bihar, and Madhya Pradeshcontinue to struggle with higher mortality ratios due to systemic lags.
Persisting Challenges
Despite a robust policy framework, several "last-mile" hurdles remain:
- High Out-of-Pocket Expenses (OOPE): Even in public facilities, families often pay for diagnostics and medicines, deterring the poorest from seeking timely emergency care.
- Socio-Cultural Barriers: Low female literacy, restricted autonomy in decision-making, and gender-based discrimination often delay the "three delays": delay in seeking care, reaching the facility, and receiving treatment.
- The New Risk Profile: Increasing instances of obesity, gestational diabetes, and hypertension, combined with delayed childbirth, are giving rise to more "high-risk" pregnancies.
- Infrastructure Gaps: Remote tribal and hilly terrains lack Emergency Obstetric Care (EmOC) and reliable blood storage units.
Government Framework & Innovations
The Government of India has launched a multi-tiered strategy to tackle MMR:
Central Schemes
- Janani Suraksha Yojana (JSY): A 2005 demand-side intervention providing cash incentives for institutional deliveries.
- PMMVY & Mission Shakti: Provides ?5,000 for the first child and an additional incentive for the second child if it is a girl, addressing both nutrition and sex ratio.
- PMSMA (9th of every month): Guarantees free, high-quality antenatal care (ANC) for all pregnant women in their 2nd/3rd trimesters.
- LaQshya: Focuses specifically on the quality of care in labor rooms and maternity OTs to prevent facility-based infections and complications.
State-Level Best Practices
- Tamil Nadu’s Referral Model: A gold standard in emergency obstetric care with a seamless ambulance and hospital linkage.
- Madhya Pradesh’s ‘Dastak Abhiyan’: Uses community health workers for early identification of high-risk pregnancies at the doorstep.
The Road to 2030
To reach the SDG target of 70 per 1,00,000, India must shift focus from "quantity" (number of deliveries) to "quality of care."
- Specialist Training: Expanding programs like LSAS (Anesthesia) and EmOC (Obstetric skills) for MBBS doctors to fill the gap of specialists in rural CHCs.
- Digital Tracking: Scaling the Reproductive and Child Health (RCH) portal for name-based tracking of every pregnant woman.
- Audit & Accountability: Strengthening Maternal Death Surveillance Reviews (MDSR) to identify why a death occurred and taking corrective local action.
The goal is to ensure that no woman loses her life while bringing another into the world—transforming maternal health from a privilege into a guaranteed right.
UN IGME 2025 Report on Child Mortality
- 24 Mar 2026
In News:
The United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) recently released its 2025 report, 'Levels and Trends in Child Mortality'. While the report underscores a concerning global deceleration in child survival progress since 2015, it distinguishes India as a leading global "exemplar." India’s sustained, large-scale interventions have resulted in a monumental decline in mortality rates, positioning the country as a primary driver of Southern Asia’s rapid progress.
Global Landscape: A Study in Concentration and Deceleration
The report reveals that despite a 50% reduction in under-five deaths since 2000, the pace of improvement has slowed by 60% since 2015.
- The Burden: In 2024, approximately 4.9 million children died before age five, with 2.3 million (nearly 50%) occurring in the neonatal period (first 28 days).
- Geographic Disparity: Mortality remains heavily concentrated in Sub-Saharan Africa (58%) and Southern Asia (25%).
- Malnutrition as a Primary Driver: For the first time, the report integrated direct causes, identifying Severe Acute Malnutrition (SAM) as the direct cause of 5% of deaths among children aged 1–59 months, though its indirect impact as an immunity-weakener is far greater.
- Adolescent Risks: The report highlights a shift in mortality causes for the 5–24 age group—girls aged 15–19 primarily succumb to self-harm, while boys in the same bracket die mostly in road accidents.
India’s Performance: Statistical Milestones
India’s progress has outpaced the Southern Asian regional average (32.8 per 1,000 live births), reflecting a robust transition in public health.
|
Indicator |
1990 Status |
2024 Status |
% Decline |
|
Under-5 Mortality Rate (U5MR) |
127 / 1,000 |
26.6 / 1,000 |
~79% |
|
Neonatal Mortality Rate (NMR) |
57 / 1,000 |
16.7 / 1,000 |
~70% |
|
Infant Mortality Rate (IMR) |
- |
23.3 / 1,000 |
- |
|
Maternal Mortality Ratio (MMR) |
130 / Lakh (2014) |
97 / Lakh |
Within reach of SDG target (<70) |
Key Drivers of India’s Success
India’s "Exemplar" status is attributed to a multi-layered strategy focusing on institutionalization and grassroots delivery:
- Institutional Deliveries: Schemes like Janani Suraksha Yojana (JSY) and JSSK have incentivized hospital births, ensuring skilled attendance.
- Specialized Care Infrastructure: The expansion of Special Newborn Care Units (SNCUs) and the Tele-SNCU hub-and-spoke model have provided critical care in remote areas.
- Preventive Interventions: Mission Indradhanush under the Universal Immunization Programme (UIP) has closed the gap in vaccine coverage.
- Nutritional Legal Framework: The National Food Security Act (2013) and POSHAN Abhiyaan address the biological "silent multiplier" of mortality—malnutrition.
- Grassroots Management: The IMNCI protocol empowers ASHA and Anganwadi workers for early diagnosis of pneumonia and diarrhea.
Persistent Challenges and Structural Bottlenecks
Despite the accolades, the "last mile" to achieving SDG 3.2 (U5MR < 25; NMR < 12) remains steep:
- The Neonatal Bulge: 63% of India's under-five deaths occur in the first 28 days. Prematurity and birth asphyxia require high-quality intrapartum care (care during labor), which remains inconsistent.
- The Malnutrition-Anemia Loop: 52.2% of pregnant women in India are anemic (NFHS-5), leading to low-birth-weight babies with compromised immunity.
- Regional and Social Inequality: While Kerala and Tamil Nadu mirror developed nations, the "BIMARU" states (UP, Bihar, MP, Rajasthan) face infrastructure deficits and social barriers like low maternal education and poverty.
- WASH Deficits: Post-neonatal deaths are still driven by pneumonia and diarrhea, linked to inadequate Water, Sanitation, and Hygiene (WASH) infrastructure in rural belts.
The Way Forward: Strategic Recommendations
To meet the 2030 SDG targets, India must double its current pace of progress:
- Focus on the "Golden Minute": Intensify training for frontline staff in neonatal resuscitation and promote Kangaroo Mother Care (KMC) and Breast Milk Banks.
- Quality over Access: Shift focus from mere institutional delivery to "Quality of Care" through the LaQshya program to improve labor room standards.
- Nutritional Quality: Transition POSHAN 2.0 focus from calorie-centrism to micronutrient density and the "First 1,000 Days" window.
- Aspirational District Strategy: Divert resources and mobile health units to tribal and remote areas to eliminate the "Golden Hour" delay in emergency pediatric care.
- Digital Integration: Scale the U-WIN platform for real-time immunization and health tracking.
Conclusion
India’s journey from a high-burden nation to a "global exemplar" is a testament to the power of targeted public health policy. However, child survival is not merely a medical goal but a prerequisite for realizing India’s demographic dividend. Achieving a converged approach across Health, Nutrition, and WASH sectors will be the final step in breaking the cycle of mortality and ensuring every child survives and thrives.
Health Security and National Security Cess Bill, 2025

- 07 Dec 2025
In News:
Parliament has passed the Health Security and National Security Cess Bill, 2025, introducing a new fiscal instrument aimed at generating dedicated resources for public health and national security. The cess will be imposed only on demerit goods such as pan masala and other notified products, and not on essential commodities.
Rationale Behind the Cess
The government argues that both public health and national security face rising fiscal pressures. Lifestyle-related diseases, particularly those linked to tobacco and similar products, impose heavy healthcare costs, while modern defence requirements involve capital-intensive investments in areas such as precision weaponry, autonomous systems, cyber and space capabilities.
By taxing demerit goods, the cess serves a dual objective:
- Deterrence – discouraging consumption of products harmful to health.
- Resource mobilisation – generating predictable funding streams for priority sectors.
This approach reflects the principle of “sin taxation”, where social costs of harmful goods are internalised through higher taxation.
Key Features of the Cess
1. Applicable Only on Demerit Goods: The cess will not affect essential household items. Goods such as pan masala, associated with high public health risks, are the primary targets.
2. Capacity-Based Levy: Unlike GST, which is consumption-based, this cess will be machine-linked and capacity-based, levied on manufacturing capacity rather than output. This system is intended to reduce tax evasion in sectors with historically weak compliance.
3. Revenue Sharing with States: A significant feature is that a portion of the cess proceeds will be shared with States, particularly for health-related schemes and awareness programmes. This is notable because traditional cesses are usually not shareable, raising earlier concerns about fiscal centralisation.
4. No Impact on GST Framework: The government clarified that the cess operates independently of the GST system. Pan masala, for instance, already attracts the highest GST slab (28%) along with compensation cess. The new cess will not alter GST revenue-sharing arrangements.
Support and Justifications
Supporters in Parliament argued that the cess ensures transparent utilisation of funds and aligns taxation with national priorities. By linking taxation to harmful goods, it seeks to create a healthier society while strengthening defence preparedness. The government emphasised that stable funding is essential in an era of rapidly evolving security threats.
Concerns and Criticisms
Opposition members raised several issues:
- Impact on MSMEs: Capacity-based taxation may burden small manufacturers with compliance costs.
- Fear of “Inspector Raj”: Increased inspections to assess production capacity could lead to bureaucratic overreach.
- Federalism Concerns: Critics described the growing use of cesses as “cessification of governance,” arguing it bypasses the divisible pool of taxes.
- Policy Effectiveness: Some MPs suggested that outright bans on harmful products might be more effective than taxation alone.
Conclusion
The Bill represents an innovative attempt to align fiscal policy with public health and national security objectives. While it signals a move toward targeted taxation and earmarked spending, its success will depend on transparent implementation, minimal compliance burden, and cooperative federalism. Balancing deterrence, revenue mobilisation, and ease of doing business will be key to ensuring that the cess achieves its intended social and strategic outcomes.
Declining Health of Parliamentary Democracy in India

- 01 Dec 2025
In News:
India’s Parliament, constitutionally envisaged as the “grand inquest of the nation”, is increasingly witnessing signs of institutional fatigue. As the Winter Session reconvenes amid controversies such as the Special Intensive Revision (SIR) of electoral rolls, concerns over legislative dysfunction, shrinking deliberation, and executive dominance have resurfaced. This decline is not episodic or partisan, but structural and long-term, threatening the balance of power central to parliamentary democracy.
Empirical Evidence of Decline
Data from PRS Legislative Research reveal a worrying trend. During a recent Monsoon Session, the Lok Sabha functioned for only 29% of its scheduled time and the Rajya Sabha for 34%. Question Hour—the most potent accountability mechanism—was particularly eroded, with the Lok Sabha completing only 23% and the Rajya Sabha merely 6% of its allotted time.
Equally concerning is the rushed passage of legislation. Major Bills such as the Regulation of Online Gaming Bill and the Merchant Shipping Bill were cleared with only minutes of discussion, undermining the deliberative purpose of Parliament under Article 107. Committee scrutiny has weakened sharply: while over 60% of Bills were referred to committees in the 14th and 15th Lok Sabhas, this figure fell to about 20% in the 16th and 17th.
The number of sittings has also declined dramatically. From an average of 121 days per year (1952–1970), Parliament now meets for about 68 days, with the 17th Lok Sabha averaging just 55 days, the lowest in independent India. Notably, it was also the first Lok Sabha without a Deputy Speaker, despite Article 93 mandating the post.
Structural Causes
A key driver of institutional erosion is the Anti-Defection Law. Intended to curb political instability, it has instead suppressed legislative independence, converting MPs into bound agents of party whips. This distorts core parliamentary functions such as:
- Power of the purse, where financial scrutiny becomes ritualistic.
- Impeachment proceedings, where MPs should act as impartial jurors rather than whipped voters.
Simultaneously, executive dominance has grown. Opposition notices, adjournment motions, and demands for discussion are frequently disallowed, forcing protests and disruptions. Presiding officers, constitutionally expected to be neutral, are increasingly perceived as partisan, further weakening trust in parliamentary conventions.
Comparative Perspective
India’s parliamentary system draws from the Westminster model, whose roots lie in the Oxford Parliament of 1258, which subordinated executive power to legislative oversight. In countries like the UK, Prime Minister’s Questions, strong committee systems, and mandatory executive testimony preserve accountability. India, by contrast, has moved in the opposite direction—towards a Parliament that often approves rather than scrutinises.
Way Forward
Reversing this decline requires deliberate reforms:
- Mandating minimum sittings (e.g., 120 days annually) to prevent rushed law-making.
- Compulsory committee referral for all major Bills.
- Reforming the Anti-Defection Law, limiting whips to confidence motions and Money Bills.
- Restoring Question Hour and Zero Hour as non-negotiable accountability tools.
- Institutionalising a Prime Minister’s Question Hour and strengthening executive accountability to committees.
- Upholding neutrality of constitutional offices, including timely election of the Deputy Speaker.
Conclusion
The decline of Parliament is not merely about productivity statistics but about the hollowing out of constitutional spirit. Without urgent corrective measures, India risks reducing Parliament to a symbolic edifice—standing tall, yet silent in its duty to hold power accountable to the people. Reviving parliamentary democracy is thus essential for preserving the republic’s constitutional balance and democratic legitimacy.
Belem Health Action Plan Launched at COP30

- 19 Nov 2025
In News:
The 30th UN Climate Change Conference (COP30) held in Belém, Brazil, marked a major turning point in global climate governance by placing human health at the centre of climate adaptation discourse. The launch of the Belém Health Action Plan (BHAP) and the announcement of a $300 million commitment by over 35 global philanthropies under the Climate and Health Funders Coalition represent the first coordinated global effort to link climate adaptation finance with public health outcomes. This shift acknowledges that climate change is no longer an environmental issue alone but a multidimensional crisis with profound implications for human health, equity and development.
Climate-linked health risks have intensified sharply, as highlighted in the 2025 Lancet Countdown Report on Health and Climate Change. Heat-related deaths have increased by 23% since the 1990s, reaching 546,000 annually. Wildfire smoke contributed to 154,000 deaths in 2024, while dengue transmission potential has risen by 49% since the 1950s. According to Lancet findings, 3.3 billion people are at heightened health risk from rising temperatures, pollution, extreme rainfall, water scarcity, vector-borne diseases and extreme events. These impacts disproportionately affect vulnerable groups—children, pregnant women, elderly people, outdoor workers and communities with fragile health systems—worsening global health inequities.
In this context, the Belem Health Action Plan, endorsed by more than 80 countries and organisations, seeks to build climate-resilient, equitable and adaptive health systems. The BHAP outlines five key focus areas:
(1) strengthening surveillance and early-warning systems for heatwaves, floods, extreme weather and infectious diseases;
(2) accelerating research and innovation in climate-sensitive health risks and technologies;
(3) promoting health equity and justice by protecting vulnerable communities;
(4) building capacity in healthcare workforces for climate-related emergencies; and
(5) aligning health, climate, and development policies for coherent action.
A core emphasis of the plan is “shifting funding and power to frontline communities,” ensuring that adaptation resources directly reach the most affected.
The $300 million philanthropic commitment complements the BHAP by supporting integrated climate-health solutions. This inaugural funding tranche will prioritize extreme heat mitigation, expansion of early-warning systems, reduction of air pollution, and improved management of climate-sensitive diseases such as malaria, dengue and cholera. A major component involves integrating climate and health data platforms, enabling real-time forecasting and targeted responses. The initiative also stresses the urgency of action, with the past decade recorded as the hottest in human history, and projections indicating continued extreme temperatures.
However, COP30 also highlighted a persistent adaptation finance gap, especially for health-focused interventions. The UN Adaptation Gap Report (2025) estimates that developing countries will require $310–365 billion annually by 2035 to meet adaptation needs, while current global flows average just $40 billion per year. Health-related adaptation receives an even smaller share. India’s 2023 National Communication to the UNFCCC projects a need for $643 billion by 2030 for adaptation, though the country has significantly scaled up domestic spending to $146 billion (5.6% of GDP) in 2021–22.
The Belem outcome reflects a paradigm shift—viewing climate adaptation not merely as environmental protection but as safeguarding human lives, livelihoods and health systems. By institutionalising a climate-health framework, strengthening collaborations between governments, global agencies and philanthropies, and expanding financing avenues, COP30 has laid the foundation for a more people-centred climate agenda. The challenge now lies in rapidly operationalising BHAP’s strategies at national and local levels, ensuring robust funding, and building resilient health systems capable of withstanding an increasingly volatile climate future.
India’s Mental Health Crisis: Towards a Unified and Inclusive Response
- 11 Oct 2025
In News:
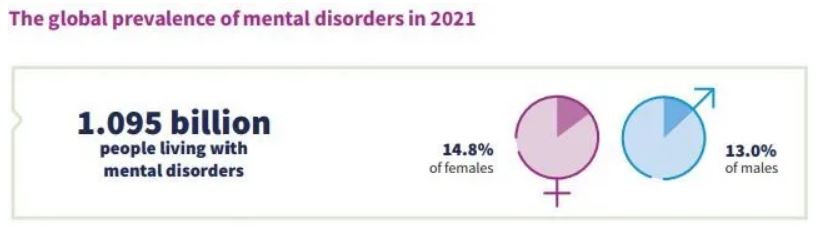
Every year on October 10, the world observes World Mental Health Day to underscore the growing burden of mental disorders — now affecting over one billion people globally, or 13% of the world’s population. India mirrors this crisis, with a 13.7% lifetime prevalence of mental disorders and rising suicides — 1.71 lakh cases in 2023, including a concerning 65% increase in student suicides over the past decade.
Rising Mental Health Concerns
Globally, anxiety and depression account for two-thirds of all diagnosed mental disorders. Between 2011 and 2021, the number of people with mental disorders rose faster than the world’s population. In India, changing social structures, excessive internet and social media use, academic pressure, and hostile work environments have aggravated psychological distress, especially among the youth. Poor lifestyle habits, reduced family interaction, and economic uncertainty have further deepened the crisis.
Structural Challenges in India’s Mental Healthcare System
India’s mental health system suffers from a triple deficit — of funding, workforce, and governance.
- Budgetary neglect: Mental health receives barely 1.05% of India’s total health expenditure, far below the WHO-recommended 5%.
- Severe workforce shortage: There are only 0.75 psychiatrists and 0.12 psychologists per 1 lakh people, compared to the WHO’s requirement of at least three psychiatrists.
- Treatment gaps: The National Mental Health Survey (2015–16) found 70–92% treatment gaps, meaning most people receive little or no professional care.
- Urban-rural divide: Specialists and rehabilitation facilities are concentrated in cities, while rural India, home to 70% of the population, remains severely underserved.
- Poor infrastructure and stigma: Many psychiatric institutions are plagued by neglect, while deep-rooted social stigma still equates mental illness with personal weakness.
Policy Framework and Initiatives
India has made several progressive policy moves:
- The Mental Healthcare Act, 2017decriminalised suicide attempts, guaranteed the right to mental healthcare, and introduced advance directives allowing patients to choose their treatment.
- The Rights of Persons with Disabilities Act, 2017recognises mental illness as a disability, expanding legal protections.
- In SukdebSaha vs. State of Andhra Pradesh, the Supreme Court affirmed mental health as part of the Right to Life under Article 21, legally obligating the state to ensure quality, accessible care.
- The District Mental Health Programme (DMHP) now operates in 767 districts, providing counselling, suicide prevention, and outreach services.
- The National Tele Mental Health Programme (Tele MANAS), launched in 2022, has enabled over 20 lakh tele-counselling sessions, improving access in underserved areas.
- Initiatives like Manodarpan aim to promote psychological well-being among over 11 crore students.
Learning from Global Models
Countries like Australia, Canada, and the UK allocate 8–10% of their health budgets to mental health and employ mid-level mental health providers who deliver nearly half of all counselling services. These nations also ensure near-universal insurance coverage and maintain real-time mental health surveillance — areas where India still lags.
Way Forward
A unified and decentralised mental health strategy must focus on:
- Raising mental health spending to at least 5% of total health expenditure.
- Expanding and training mid-level providers to bridge the rural-urban gap.
- Fully integrating mental health into primary healthcare and insurance systems.
- Updating diagnostic and policy frameworks in line with WHO’s ICD-11.
- Establishing district-level monitoring and accountability systems.
- Scaling anti-stigma campaigns across schools, workplaces, and communities.
- Ensuring inter-ministerial coordination among health, education, social justice, and labour departments for a cohesive national response.
Conclusion
India’s mental health challenge is not merely a medical issue but a socio-economic and governance imperative. Bridging systemic gaps in funding, workforce, and awareness—while fostering empathy and inclusion—can transform India’s mental health landscape, aligning it with global best practices and the vision of holistic well-being under Article 21 of the Constitution.
Childhood Obesity in India: A Growing Public Health Challenge

- 14 Jun 2025
Introduction
Childhood obesity has emerged as a serious public health concern in India, mirroring global trends. A recent study places India among the top countries grappling with rising obesity among children. This phenomenon, once limited to affluent sections, is now widespread across urban and semi-urban regions, driven by a complex interplay of dietary, behavioural, genetic, and socio-economic factors.
Understanding the Causes
- Dietary Shifts and Unhealthy Eating Habits: The increasing consumption of calorie-dense, ultra-processed foods, sugary beverages, and fast food is one of the primary contributors to childhood obesity. Traditional, balanced home-cooked meals are being replaced due to changing family dynamics and time constraints, leading to poor nutritional choices among children.
- Sedentary Lifestyle and Screen Time: The decline in physical activity among children is alarming. Excessive screen exposure through television, mobile phones, and video games, coupled with a lack of safe outdoor spaces and diminishing emphasis on physical education in schools, has led to a largely sedentary routine among adolescents.
- Genetic and Medical Predispositions: Genetic predisposition plays a significant role. Children with a family history of obesity are more susceptible. Medical conditions like hypothyroidism and insulin resistance further increase vulnerability.
Consequences of Childhood Obesity
- Physical Health Risks: Obese children are at an elevated risk of early-onset non-communicable diseases (NCDs) such as Type 2 diabetes, cardiovascular ailments, hypertension, and musculoskeletal disorders. They may also experience early puberty and related hormonal imbalances.
- Psychosocial Impact: Beyond physical health, obesity in children is linked to psychological distress. Affected children often face bullying, social exclusion, low self-esteem, and are more prone to depression and anxiety. These challenges can persist into adulthood, impacting mental well-being and social functioning.
Preventive Strategies: The Role of Family, Schools, and Policy
- Parental Involvement and Home Environment
- Promoting home-cooked nutritious meals over packaged or junk food.
- Integrating physical activities like walking, yoga, or family sports into daily routines.
- Educating children on food labels, nutrition, and healthy choices.
- Involving children in meal preparation and encouraging mindful eating practices.
- School-based Interventions
- Making physical education compulsory and structured in the school curriculum.
- Conducting regular health screenings and awareness campaigns.
- Promoting healthy food environments in school canteens and classrooms.
- Organizing workshops on nutrition, mental health, and lifestyle habits.
- Health Monitoring and Medical Intervention
- Periodic health check-ups to identify early signs of obesity and related conditions.
- Early medical and nutritional interventions to prevent progression to severe obesity or associated NCDs.
Policy Imperatives and Way Forward
Given its long-term implications on public health and healthcare burden, childhood obesity must be addressed through a multi-sectoral approach involving:
- Policy frameworks that regulate food marketing targeted at children, particularly unhealthy snacks and beverages.
- Urban planning that ensures safe public spaces for physical activity and sports infrastructure in schools.
- Integration with national health programmes like the Rashtriya Bal Swasthya Karyakram (RBSK) and POSHAN Abhiyan to monitor and support child nutrition holistically.
- Mass awareness campaigns to de-stigmatize obesity and promote healthy behaviours.
Conclusion
Childhood obesity is no longer a concern confined to individuals—it is a looming public health challenge with intergenerational consequences. If not addressed early, it risks leading to a population burdened by NCDs and compromised productivity. Collaborative action by parents, educational institutions, healthcare providers, and government agencies is critical to reversing this trend and ensuring a healthier future for India’s children.
WHO Pandemic Agreement: A Landmark Step Towards Global Health Security

- 21 May 2025
Context:
The World Health Assembly (WHA), the decision-making body of the World Health Organization (WHO), adopted the first-ever Pandemic Agreement at its 78th session in May 2025. This historic and legally binding agreement, three years in the making, aims to strengthen global pandemic preparedness, prevention, and response with a focus on equity, solidarity, and scientific evidence. Triggered by the gaps and inequities exposed during the COVID-19 crisis, the accord marks a milestone in global health governance under Article 19 of the WHO Constitution, previously used for the 2003 Framework Convention on Tobacco Control.
The agreement was unanimously approved by 124 countries, with no opposition and 11 abstentions. It emphasizes that national sovereignty remains intact, explicitly stating that WHO cannot mandate domestic laws or measures such as lockdowns, vaccine mandates, or travel restrictions. This provision addresses concerns of state overreach and promotes voluntary, collaborative international action.
A central feature is the creation of a Pathogen Access and Benefit Sharing (PABS) system, wherein countries that share virus samples will receive equitable access to vaccines, diagnostics, and therapeutics. Participating pharmaceutical companies must allocate 20% of their real-time production (10% as donations, 10% at affordable prices) to WHO for distribution based on public health needs, especially in developing nations. This move addresses the vaccine nationalism witnessed during COVID-19 and promotes global health equity.
To support this system, the agreement calls for the establishment of a Global Supply Chain and Logistics Network (GSCL), coordinated by WHO, to ensure timely and fair distribution of essential health products during public health emergencies. Member states are encouraged to develop national pandemic prevention plans, improve disease surveillance, and invest in routine immunisation, antimicrobial resistance control, and zoonotic disease prevention.
Another key pillar is the promotion of sustainable local production of health products and technology transfer to developing countries. Mechanisms such as licensing, regulatory incentives, and financing are to be used to facilitate regional and global tech hubs. These efforts are aimed at reducing reliance on a few manufacturing nations and improving rapid response capabilities globally.
The agreement’s adoption is politically significant in reaffirming multilateralism amid rising nationalism. WHO Director-General Dr. Tedros Adhanom Ghebreyesus hailed it as a “victory for public health and multilateral cooperation.” However, the absence of the United States — a major global health funder and former leader in pandemic response — casts a shadow. The U.S. withdrew from the drafting process following the Trump administration’s move to exit WHO, raising concerns about the treaty’s universality and enforcement.
Despite the lack of a penalty mechanism for non-compliance, the agreement represents a global consensus on shared responsibility for health security. It acknowledges that pandemics pose transboundary risks requiring coordinated international action, especially to protect vulnerable populations and frontline workers.
Expected to enter into force after ratification by 60 countries and the finalisation of PABS and GSCL mechanisms by May 2026, the WHO Pandemic Agreement is a pivotal step in ensuring the world is better prepared, more resilient, and more just in the face of future pandemic threats.
Mental Health Insurance Coverage in India
- 09 May 2025
Context:
Mental health insurance coverage in India remains critically inadequate despite rising awareness of mental health issues. According to the RiseUP for a Better Tomorrow: Mental Health Report 2025, mental health accounts for less than 1% of total health insurance claims, reflecting a glaring disparity in healthcare priorities. This neglect persists despite a robust legal and regulatory framework aimed at promoting mental health coverage.
The Mental Healthcare Act, 2017 legally mandates that mental health be treated on par with physical health in insurance policies. In line with this, the Insurance Regulatory and Development Authority of India (IRDAI) issued guidelines in 2019 requiring insurers to include mental health illnesses in coverage plans. However, implementation remains patchy, especially in group insurance policies. Many plans continue to exclude essential mental health services, undermining legislative intent.
Current insurance offerings are heavily skewed towards hospitalization for severe mental illnesses, with minimal coverage for outpatient care—counselling, therapy, and medication—which forms the backbone of mental healthcare. Only 17% of insured individuals have access to outpatient mental health services. Additionally, schemes like Ayushman Bharat offer limited support for mental health, and common exclusions such as substance abuse and self-inflicted injuries reduce the scope of coverage.
On the demand side, awareness is a significant barrier. Around 42% of people are unaware of their mental health coverage, while 83% of organizations report low utilization of mental health insurance. Out-of-pocket expenses still account for 60–70% of mental healthcare costs (NMHS 2015–16), adding to the economic burden. A staggering 70–90% of individuals with mental disorders remain untreated, largely due to poor insurance access.
From the supply perspective, policy design is often modeled on physical health, failing to account for the chronic and outpatient nature of many mental health conditions. Nearly 50% of respondents in the RiseUP report cited high treatment costs as a deterrent to seeking care, a concern aggravated by restrictive policies and long claim settlement periods. Furthermore, the limited empanelment of mental health professionals constrains access for insured individuals.
Social stigma continues to be a pervasive barrier. Nearly half of the surveyed individuals fear discrimination if their mental health needs are revealed. This stigma leads to underreporting and delays in seeking care, further deepening the treatment gap.
Government initiatives like the National Mental Health Programme (NMHP) and Tele-MANAS are promising steps but require integration with insurance mechanisms to be effective. Seamless coordination between public services and insurance schemes is crucial.
Way Forward:
There is a pressing need to redesign insurance policies to comprehensively include outpatient mental health care, increase awareness through targeted campaigns, reduce stigma through public health messaging, streamline claims processing, and expand provider networks. Regulatory bodies like IRDAI must ensure compliance through audits and penalties, while employers should be incentivized to offer robust mental health coverage.
Conclusion:
Expanding mental health insurance is vital for a healthier, more inclusive, and productive society. Achieving this calls for a multi-stakeholder approach involving legal enforcement, policy reform, public education, and systemic coordination between government and private actors.
Public Health Education in India

- 18 Mar 2025
In News:
India’s public health education sector stands at a critical juncture. Despite rapid academic expansion—with over 100 institutions now offering Master of Public Health (MPH) and related programs—the sector faces mounting challenges related to employment, quality, and funding. While international aid has declined, domestic investment remains limited, exacerbating systemic issues in workforce development.
Public Health: Constitutional and Strategic Significance
Article 47 of the Indian Constitution mandates the State to improve public health. A well-trained public health workforce is essential to achieve health equity, manage non-communicable diseases, address pandemics like COVID-19, and ensure effective delivery of health services at all levels.
Evolution and Growth of Public Health Education
Public health education in India has roots in colonial institutions, notably the All India Institute of Hygiene and Public Health, Kolkata (1932). Post-independence, community medicine was integrated into medical curricula. However, it was the launch of the National Rural Health Mission (2005) that marked a turning point, creating space for non-medical professionals in public health. Since then, MPH programs have proliferated—from just one institution in 2000 to over 100 today.
Government Initiatives
Key government efforts to strengthen public health education and training include:
- National Health Mission (NHM): Enhances public health systems and skill development.
- PM Swasthya Suraksha Yojana (PMSSY): Expands infrastructure and education through AIIMS-like institutions.
- Fellowship in Public Health Management (FPHM): Builds leadership capacities.
- National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD) and Integrated Disease Surveillance Programme (IDSP): Promote epidemiology and disease control training.
Persistent Challenges
- Employment Mismatch: A surge in MPH graduates has not been matched by job creation. Entry-level roles receive thousands of applications, and dedicated public health cadres in states remain underdeveloped.
- Lack of Regulation and Standardization: No central regulatory body ensures consistent curricula or quality standards. MPH programs are not under the purview of the NMC or UGC.
- Faculty Shortages and Weak Practical Training: Institutions often lack experienced faculty and real-world training integration, leaving graduates underprepared.
- Uneven Institutional Spread: States like Assam, Bihar, and Jharkhand have few or no public health colleges, deepening regional disparities.
- Funding Deficits: India's public health education receives minimal investment. For instance, the Data Protection Board was allocated just ?2 crore—reflecting systemic underfunding. International aid cuts, such as those from USAID, further strain the sector.
- Low Private Sector Absorption: Private hospitals prefer management professionals over MPH graduates. Development sector roles, heavily reliant on foreign grants, offer limited stability.
Way Forward
- Establish Public Health Cadres: States must create dedicated employment frameworks at all administrative levels.
- Regulate Education Quality: A Public Health Education Council under UGC/NMC should standardize curricula, faculty norms, and institutional benchmarks.
- Expand Institutional Capacity: Encourage public-private partnerships to open MPH colleges in underserved regions.
- Promote Experiential Learning: Mandate field training through internships in NHM, IDSP, and WHO-linked programs.
- Encourage Private Sector Hiring: Offer incentives for hiring MPH graduates in corporate and hospital settings.
- Increase Domestic Investment: Boost government funding for public health education and research, reducing reliance on foreign donors.
Conclusion
India’s public health education must transition from fragmented expansion to structured, quality-driven growth. Strengthening regulation, employment pathways, and training infrastructure is crucial for building a resilient health system and fulfilling the constitutional promise of health for all.
Over-Centralisation and Federal Health Governance in India

- 10 Mar 2025
Introduction
India’s health governance follows a quasi-federal structure where health is constitutionally a State subject. However, increasing centralisation, particularly in medical education and national health schemes, is raising concerns over States’ autonomy and the effectiveness of federal health policies.
Judicial Push Towards Centralisation
The recent Supreme Court ruling in Dr. Tanvi Behl vs Shrey Goyal (2025) declared domicile-based reservations in post-graduate (PG) medical admissions unconstitutional, citing Article 14 and the principle of meritocracy. This decision, however, overlooks the critical link between State investments in medical education and their ability to retain specialists within local health systems. Domicile quotas served as a strategic tool to ensure a stable, locally adapted healthcare workforce, especially amid chronic specialist shortages.
Striking down such quotas may discourage States from investing in medical institutions if their graduates are siphoned off to other regions. Unlike central institutions like AIIMS or PGIMER, which enjoy selection autonomy, State medical colleges now face limited control over admissions, weakening their role as pillars of regional health systems.
Centralisation Through Policy and Institutions
Beyond judiciary-led centralisation, several national initiatives have expanded the Centre's role:
- National Health Mission (NHM): While implemented by States, funding and guidelines remain Centre-dominated.
- Ayushman Bharat (2018) and AB Digital Mission: These schemes shifted healthcare financing and data control towards the Centre, reducing the relevance of State-run insurance programs.
- National Medical Commission Act (2019): Replacing the MCI, this law enhanced the Centre's control over medical education regulation.
- Epidemic and Disaster Management Acts: Empower the Centre during health emergencies, as witnessed during COVID-19.
Consequences of Over-Centralisation
Excessive centralisation undermines India’s diverse health needs and local governance:
- Limited Responsiveness to Local Needs: Uniform policies ignore State-specific demographics. For instance, Kerala requires elderly care, while Bihar and UP demand maternal and child health focus.
- Reduced Decision-Making Power: States lose flexibility in tailoring central schemes, as seen with Ayushman Bharat PM-JAY.
- Bureaucratic Inefficiencies: Delays in fund disbursal under centrally sponsored schemes hinder timely execution.
- Weakening of Local Health Systems: Panchayats and municipal bodies—crucial to grassroots delivery—are often bypassed in favour of top-down mechanisms.
Meritocracy vs Social Equity
The rigid focus on merit in PG admissions disregards structural inequalities. As seen in recent NEET-PG cutoffs being lowered to zero percentile to fill seats, the current meritocratic model is flawed. Regional representation and public service outcomes should be considered in defining ‘merit’, aligning medical education with societal needs.
Way Forward
- Restore State Autonomy in Admissions: States should be empowered to design admissions aligned with local healthcare priorities.
- Fiscal and Functional Decentralisation: Grant flexibility in using central funds and reduce bureaucratic controls.
- Strengthen Cooperative Federalism: Institutionalise Centre-State coordination in health planning and policy-making.
- Invest in Local Systems: Enhance capacities of State health departments and grassroots governance bodies.
Conclusion
While central guidance is essential for national health objectives, excessive centralisation risks weakening India’s federal health architecture. A balanced approach rooted in cooperative federalism is vital to create an inclusive, efficient, and resilient healthcare system for all.
Mental Health in India: Budget 2025–26

- 06 Feb 2025
In News:
The Union Budget 2025–26 marks a pivotal step towards strengthening mental health infrastructure in India. An allocation of ?99,858.56 crore to the Ministry of Health and Family Welfare (MoHFW) highlights the government’s recognition of health, including mental health, as a key pillar of national development.
Key Budgetary Allocations for Mental Health (2025–26)
- National Tele Mental Health Programme (NTMHP): Allocated ?79.6 crore to expand access to mental health services across the country.
- National Institute of Mental Health and Neurosciences (NIMHANS): Receives support to enhance research and treatment capacity.
- District Mental Health Programme: Implemented in 767 districts, providing training and outpatient services.
- Ayushman Arogya Mandirs: Over 1.73 lakh SHCs and PHCs are being upgraded to offer mental health services under comprehensive primary care.
Mental Health in India: Status and Burden
- As per WHO, mental health is the ability to realize one’s potential, cope with stress, work productively, and contribute to the community.
- India's Burden:
- 15% of adult Indians experience mental disorders (National Survey).
- Mental morbidity is highest in urban metros (13.5%), followed by rural areas (6.9%) and non-metro urban zones (4.3%).
- Global Burden (2019): Around 970 million people globally suffered from mental disorders, notably anxiety and depression.
- Treatment Gap: Estimated at 70% to 92%, particularly acute among blue-collar workers.
- Economic Impact: Mental health disorders result in significant productivity losses, often surpassing the direct cost of care.
Challenges in Mental Health Care in India
1. Budgetary and Policy Limitations
- The National Mental Health Programme (NMHP) faces funding ambiguities, often subsumed under broader health allocations.
- Limited enforcement of Mental Healthcare Act, 2017, despite mental health being a statutory right. Over 11 crore Indians suffer from mental disorders, yet 80% do not seek help.
2. Exclusion in Labour Laws
- The Occupational Safety, Health and Working Conditions Code (OSHWC), 2020, primarily covers physical safety. Mental health is not explicitly recognized.
- Phrases like “as far as reasonably practicable” limit employers’ obligations.
- The Code on Social Security (CSC), 2020, does not list mental strain as an occupational disease, making compensation for stress-induced conditions difficult.
3. Neglect of Blue-Collar Mental Health
- Mental health risks—long hours, poor conditions, job insecurity—affect blue-collar workers disproportionately.
- Workplace mental health programs (e.g., Infosys HALE, TCS EAP) are mainly for white-collar employees.
- Tele-MANAS, a government mental health helpline, requires voluntary calls. Low awareness and stigma among blue-collar workers dilute its effectiveness.
Policy and Structural Reforms Needed
- Legislative Frameworks:
- Amend OSHWC and CSC to explicitly include mental well-being and stress-related injuries as compensable conditions.
- Update the Third Schedule of the CSC to include mental health conditions, reducing dependence on case law.
- Awareness and Education:
- Launch mandatory employer-led awareness campaigns on programs like Tele-MANAS and Manodarpan.
- Community-based programs for early detection, support, and referral of mental health disorders.
- Inclusive and Tripartite Approach:
- Integrate employers, blue-collar workers, and mental health professionals into a unified framework under the new Labour Codes.
- Incorporate mental health indicators into occupational safety audits.
- Institutional Strengthening:
- Increase capacity-building efforts by training frontline health workers, general physicians, and non-specialist cadres in mental healthcare.
- Establish Centres of Excellence for mental health training and research.
Global and National Initiatives
- WHO Comprehensive Mental Health Action Plan (2013–2030): Focuses on integrating mental health into primary care and strengthening community-level interventions.
- Manodarpan Initiative: Aims at student mental health support under Atmanirbhar Bharat.
- Kiran Helpline: Government-run suicide prevention helpline for crisis support.
- Tele-MANAS Cells: 53 centers operational in 36 States/UTs, enhancing digital mental health care access.
Conclusion and Way Forward
The 2025–26 Budget reflects a progressive approach to mental health, particularly through investments in tele-counselling, primary care, and institutional support. However, significant gaps remain in policy, especially in addressing the mental health needs of blue-collar workers.
To transform “Satyamev Jayate” to “Shramev Jayate,” India must:
- Institutionalize rights-based mental health protection in labour legislation.
- Close the treatment gap through universal access and community-level awareness.
- Recognize mental health as integral to human capital and national productivity.
Only a comprehensive, inclusive, and rights-oriented approach will ensure mental health equity in India’s development journey.
National Health Mission (NHM): 2021–2024

- 24 Jan 2025
In News:
The Union Cabinet reviewed the progress under NHM (2021–24), underscoring significant gains in public health infrastructure, disease control, and healthcare accessibility, particularly during and after the COVID-19 pandemic.
About NHM:
- Launched: 2013, integrating NRHM (2005) and NUHM (2012).
- Objective: Universal access to equitable, affordable, and quality healthcare services.
- Focus: Vulnerable populations, rural and urban poor.
- Implementation: Ministry of Health & Family Welfare supports states and UTs.
Key Achievements (2021–2024):
1. Human Resource Expansion
- 12.13 lakh healthcare workers added, including doctors, nurses, CHOs, and AYUSH practitioners.
- Ni-kshay Mitras: 1.56 lakh volunteers supported 9.4 lakh TB patients.
- Progressive annual engagement:
- FY 2021–22: 2.69 lakh
- FY 2022–23: 4.21 lakh
- FY 2023–24: 5.23 lakh
Maternal and Child Health
- Maternal Mortality Ratio (MMR): Dropped by 83% since 1990 (from 130 to 97 per lakh live births).
- Under-5 Mortality Rate (U5MR): Reduced from 45 (2014) to 32 (2020).
- Infant Mortality Rate (IMR): Declined from 39 (2014) to 28 (2020).
- Total Fertility Rate (TFR): Reduced from 2.3 (2015) to 2.0 (2020).
Disease Control and Elimination
- Tuberculosis (TB):
- Incidence: From 237 (2015) to 195 (2023) per 1,00,000.
- Mortality: Decreased by 21.4% (from 28 to 22).
- Kala-azar: Target achieved in all endemic blocks (<1 case/10,000 population by 2023).
- Sickle Cell Anemia: 2.61 crore people screened under the National Elimination Mission.
- Malaria:
- Cases fell in 2021 but rose in 2022 and 2023.
- Deaths declined continuously.
Immunization Campaigns
- COVID-19: Over 220 crore doses administered (2021–2024).
- Measles-Rubella: 97.98% coverage, vaccinating 34.77 crore children under IMI 5.0.
- Digital Health: U-WIN platform launched in 2023 for real-time vaccination tracking in 65 districts.
Healthcare Infrastructure
- 7,998 health facilities certified under National Quality Assurance Standards (NQAS).
- Ayushman Arogya Mandirs: 1.72 lakh operational, with 1.34 lakh offering 12 essential services.
- 24×7 services: At 12,348 PHCs and 3,133 FRUs.
- Mobile Medical Units (MMUs): Expanded to 1,424 units, MMU Portal operational.
Specialized Health Initiatives
- Pradhan Mantri TB Mukt Bharat Abhiyan: Volunteer-driven TB patient support.
- Pradhan Mantri National Dialysis Programme:
- Delivered 62.35 lakh hemodialysis sessions to 4.53 lakh patients in FY 2023–24.
- Sickle Cell Mission: Major tribal health initiative targeting elimination by 2047.
National Programs Under NHM
- RMNCH+A: Reproductive, Maternal, Newborn, Child, and Adolescent Health.
- Communicable Disease Control: TB, malaria, leprosy, HIV/AIDS.
- Non-Communicable Diseases (NCDs): Cancer, diabetes, hypertension.
- Other Initiatives: Rashtriya Bal Swasthya Karyakram (RBSK), PM National Dialysis Programme, Ayushman Bharat (AB-PMJAY).
Alignment with SDG Goals
- NHM achievements indicate India is on track to meet SDG-3 targets (Good Health and Well-being), especially in maternal and child mortality reduction.
The Mental Health Crisis in India

- 10 Oct 2024
In News:
India faces a significant mental health crisis, driven by various factors including economic disparities, social isolation, and changing family dynamics. The pandemic further worsened these issues, leading to detrimental effects on mental well-being.
Causes of Mental Illness
- Socioeconomic Factors: Poverty, violence, inequality, and environmental deprivation contribute to rising mental health issues.
- Pandemic Impact: Lockdowns and uncertainties have heightened stress levels and anxiety.
- Adverse Life Experiences: Trauma, abuse, and dysfunctional family relationships can severely impact mental health.
- Cultural Pressures: The urban focus on consumerism and status can lead to feelings of inadequacy and dissatisfaction.
The Shortage of Mental Health Professionals
India's mental health services are severely lacking, with only 0.75 psychiatrists per 100,000 population—far below the World Health Organization's recommendation of three. This shortage underscores the need for policy interventions and incentives to increase the supply of mental health professionals.
Government Initiatives for Mental Health
The Indian government has implemented several initiatives to improve mental health care:
- National Mental Health Programme (NMHP): Launched in 1982 to enhance community-based mental health services.
- Mental Healthcare Act, 2017: Decriminalized suicide attempts and introduced advanced directives for treatment choices.
- Rights of Persons with Disabilities Act, 2017: Recognizes mental illness as a disability, enhancing rights for affected individuals.
- Manodarpan Initiative: Provides psycho-social support to students.
- Kiran Helpline: A suicide prevention helpline for crisis management.
- National Tele-Mental Health Programme: Launched in 2022 to expand access to mental health services, particularly in underserved areas.
Economic Survey 2023-24
For the first time, the Economic Survey emphasized the importance of mental health in policy recommendations, calling for effective implementation of mental health initiatives to address existing gaps.
Understanding Healthy Workplaces
Defining a Healthy Workplace
A healthy workplace fosters collaboration between employers and employees to promote physical and psychological safety. It encompasses open communication, respect, and a supportive environment, crucial for addressing workplace stress, anxiety, and burnout.
Current Crisis: Overwork and Mental Health
The phenomenon of ‘Karoshi’ (death from overwork) highlights the severe consequences of workplace stress. In India, 40% of employees report high stress levels due to excessive work demands.
Ethical Perspectives on Healthy Workplaces
Creating a healthy workplace involves:
- Fairness and Equity: Ensuring all employees have equal access to resources and opportunities.
- Respect for Individual Dignity: Acknowledging contributions and fostering psychological safety.
- Moral Responsibility of Employers: Providing a safe working environment and promoting mental health initiatives.
- Transparency and Accountability: Building trust through open communication about policies and practices.
- Promoting Work-Life Balance: Encouraging a balance between professional and personal life to prevent burnout.
Global Precedents for Work-Life Balance
Countries like Australia and France have introduced regulations, such as the ‘right to disconnect,’ allowing employees to disengage from work communications after hours.
Conclusion and Way Forward
Establishing healthy workplaces is not merely a regulatory compliance issue but an ethical commitment to employee well-being. Both employers and employees must collaborate to create an environment of psychological safety, open communication, and mutual respect. By prioritizing these principles, organizations can foster workplaces that enhance productivity and support mental health, ultimately driving innovation and improving overall well-being.
Shaping India’s path to inclusive health care

- 08 Apr 2024
Why is it in the News?
World Health Day, which is observed every year on April 7, unites us around health equity, an essential topic at the heart of global health and justice.
Context:
- World Health Day, commemorated every April 7th, underscores the significance of health equity, acknowledged as a basic human entitlement by the World Health Organization (WHO).
- Hence, it is imperative to delve into the theme "My Health, My Right," delving into the hurdles and remedies in attaining health equity in India.
- As a country contending with multifaceted socioeconomic inequalities in healthcare access and results, this exploration becomes pivotal.
What is Health Equity?
- Health equity, as outlined by the WHO, embodies the principle that every person should have the opportunity to attain optimal health, irrespective of their social, economic, or environmental circumstances.
- It extends beyond mere healthcare access, addressing underlying factors such as poverty, discrimination, and resource imbalances.
- Considering Diverse Health Outcomes: A core tenet of health equity acknowledges that health results stem from a multifaceted interplay of elements, encompassing social, economic, and environmental determinants.
- Individuals from disadvantaged backgrounds often encounter obstacles like financial constraints, transportation limitations, and sparse healthcare facilities.
- The Vitality of Health Equity: Health equity holds paramount importance not only ethically but also from a public health standpoint.
- Research consistently indicates that societies fostering greater health equity typically enjoy superior health outcomes, marked by lower morbidity and mortality rates, reduced healthcare expenditures, and heightened life expectancy.
- Conversely, persistent health disparities may precipitate societal unrest, economic strains, and a squandered human potential.
Health Equity Challenges in India:
- Addressing Urban-Rural Disparities: India contends with pronounced healthcare inequalities between urban and rural regions, where urban areas typically boast superior healthcare infrastructure and services, while rural communities encounter obstacles like limited access to facilities, healthcare professionals, and infrastructure, resulting in inferior health outcomes compared to their urban counterparts.
- Navigating Overcrowded Urban Slums: Urban slums present profound challenges characterized by extreme poverty, overcrowding, unsanitary conditions, and inadequate access to clean water, fostering the spread of infectious diseases and escalating morbidity and mortality rates.
- Moreover, deficient healthcare infrastructure exacerbates health disparities as residents grapple with limited access to essential services.
- Tackling Socioeconomic and Caste Disparities: Marginalized groups, including Scheduled Castes, Scheduled Tribes, and economically disadvantaged populations, confront elevated rates of illness and death due to restricted healthcare access, diminished health literacy, and societal prejudice.
- These disparities intertwine with broader determinants like education, employment, and housing, perpetuating disparities in health outcomes.
- Confronting the Burden of Non-Communicable Diseases (NCDs): Non-communicable diseases (NCDs) such as cardiovascular ailments, diabetes, and cancer pose a mounting challenge to health equity in India, constituting a substantial portion of the disease burden.
- However, marginalized communities often face barriers to accessing preventive measures and NCD treatment, amplifying health inequalities and exacerbating existing socioeconomic gaps.
- Navigating Shortages in Healthcare Personnel: A severe shortage of healthcare professionals, with only 0.8 doctors per 1,000 individuals according to WHO data, exacerbates health challenges, particularly in rural areas where access to primary care is limited, resulting in delayed diagnoses, substandard treatment, and compromised health outcomes.
- Confronting Infrastructure and Resource Limitations: Inadequate healthcare infrastructure, insufficient funding, and resource limitations pose formidable obstacles to health equity in India, with many public facilities lacking essential equipment, medications, and skilled personnel.
- Furthermore, the unequal distribution of resources aggravates urban-rural healthcare disparities, exacerbating inequities in access to quality healthcare services.
Strategies and Measures to Advance Health Equity in India:
- Enhancing Primary Healthcare Services: A pivotal approach to fostering health equity in India involves bolstering primary healthcare provisions, especially in rural and marginalized regions.
- This entails augmenting the accessibility and availability of primary care facilities, fortifying the skills and capabilities of frontline healthcare personnel, and ensuring the delivery of essential health services encompassing preventive care, maternal and child healthcare, and management of chronic ailments.
- Initiatives such as the National Rural Health Mission (NRHM) and the National Urban Health Mission (NUHM) strive to extend primary healthcare access and mitigate healthcare disparities between urban and rural locales.
- Advocating for Universal Health Coverage: Universal health coverage (UHC) stands as a cornerstone in ensuring equitable access to indispensable healthcare services devoid of financial strains.
- Endeavors like Ayushman Bharat, India's flagship health insurance program, aspire to furnish financial safeguarding to vulnerable segments by offering comprehensive coverage for hospitalization expenses.
- By broadening the reach of quality healthcare services and alleviating out-of-pocket costs, UHC endeavors to redress discrepancies in healthcare accessibility and enhance health outcomes for all citizens.
- Targeting Social Determinants of Health: Attaining health equity mandates a multifaceted approach that transcends healthcare interventions to address the underlying social determinants of health, encompassing poverty, education, housing, and employment.
- Initiatives geared towards poverty mitigation, augmenting educational and sanitation access, and fostering livelihood opportunities can wield a transformative impact on health outcomes and help ameliorate health disparities.
- Programs like the Mahatma Gandhi National Rural Employment Guarantee Act (MGNREGA) furnish rural households with employment prospects, thereby fostering enhanced socioeconomic circumstances and superior health outcomes.
- Empowering through Health Literacy: Elevating health literacy assumes paramount significance in empowering individuals to make informed health decisions and pursue equitable healthcare access.
- Integration of health education within prevailing healthcare schemes can heighten public consciousness and advocate for preventive healthcare practices.
- Fostering Collaborative Endeavors: Efficacious collaboration among governmental bodies, civil society, healthcare providers, and international entities constitutes a linchpin in addressing health inequities.
- By harnessing their respective competencies and resources, these stakeholders can conceptualize culturally sensitive health initiatives tailored to the distinctive requisites of diverse communities.
Conclusion
Realizing health equity in India necessitates coordinated endeavors spanning various sectors and involving diverse stakeholders. Through targeted interventions addressing socioeconomic health determinants, bolstering healthcare infrastructure, and fostering collaborative alliances, India can progress towards a future where equitable access to superior healthcare becomes a universal norm. The pursuit of health equity transcends moral imperatives, emerging as a pivotal prerequisite for fostering sustainable development and societal advancement.
What are the Pollutants in Our Air, and How They Impact Health (Indian Express)
- 08 Nov 2023
Why is it in the News?
Rising pollution levels in north India have led to focus returning on the Air Quality Index (AQI) score, a measure of air pollution.
Context:
- The escalating pollution in northern India has once again drawn attention to the Air Quality Index (AQI) score, which gauges air pollution levels.
- On Monday, Delhi, for instance, registered an AQI score exceeding 400.
- This categorizes the air quality as 'severe,' with any reading above 100 indicating at least a moderate level of pollution on the index.
What is the Air Quality Index (AQI)?
- AQI is a number, which is a measure of air quality.
- The higher the AQI, the worse the air.
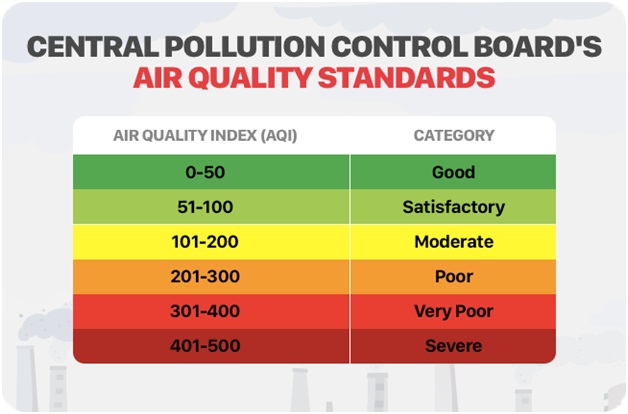
- The color-coded AQI index was launched in India in 2014, and it helps the public and the government understand the condition of the air and what subsequent measures are to be taken to combat the situation, based on its severity.
- According to the Central Pollution Control Board, part of the Ministry of Environment, Forests, and Climate Change, the AQI transforms complex air quality data of various pollutants into a single number (index value), nomenclature, and color.
- The pollutants measured include PM 10, PM 2.5, Nitrogen Dioxide, Ozone, Carbon, etc.
- There are six categories of AQI, namely ‘Good’ (0-50), ‘Satisfactory’ (51-100), ‘Moderately polluted’ (101-200), ‘Poor’ (201-300), ‘Very Poor’ (301-400), and ‘Severe’ (401-500).
How Pollutants Impact Our Health?
PM 10 and PM 2.5
- These are extremely fine particulate matter (PM) particles, with the digits accompanying them referring to their diameter.
- So, PM 10 and PM 2.5 are smaller than 10 and 2.5 microns in their diameter, respectively.
- One micron is about a thousandth of a millimeter and this tiny size has a role to play in how they impact human health.
- The finer the particles are, the more difficult it gets to protect oneself from them.
- Due to their size, the PM 2.5 particles can easily bypass the nose and throat and can enter the circulatory system.
- The particles can also lead to chronic diseases such as asthma, heart attack, bronchitis, and other respiratory problems.
- Byproducts of emissions from factories, vehicular pollution, construction activities, and road dust, such particles are not dispersed and stay suspended in the air that we breathe.
Nitrogen Dioxide (NO2)
- Nitrogen dioxide (NO2) gets in the air from the burning of fuel, with sources including emissions from vehicles and power plants.
- Short-term exposure to high levels of NO2 can aggravate respiratory diseases like asthma, and lead to other problems such as coughing or difficulty in breathing.
- Long-term exposure may also contribute to the development of asthma and could increase susceptibility to respiratory infections.
Ozone (O3)
- Ozone is a gas that is present in the upper layers of the atmosphere, protecting human health from the impact of the Sun’s UV rays.
- However, surface-level ozone is among the most significant air pollutants. It is formed by the reaction of atmospheric pollutants in the presence of sunlight.
- According to the International Journal of Medical Public Health, with the increase in surface ozone levels, there is a likelihood of an increase in the risk of hospital admissions for Chronic Obstructive Pulmonary Diseases (COPD) and the number of cardiovascular and respiratory deaths.
Sulphur Dioxide (SO2)
- The largest source of SO2 in the atmosphere is the burning of fossil fuels by power plants and other industrial facilities.
- Additional sources are industrial processes and natural sources such as volcanoes.
- As with other gases, SO2 exposure is harmful to the cardiovascular system and can lead to the development of respiratory illnesses.
- SO2 can also react with other compounds to form particulate matter.
- At high concentrations, gaseous SOx can harm trees and plants by damaging foliage and decreasing growth.
Ammonia (NH3)
- A 2017 NASA-funded study said that in India, “A broad increase in fertilizer use coupled with large contributions from livestock waste have resulted in the world’s highest concentrations of atmospheric ammonia.”
- While gaseous ammonia is a natural part of Earth’s nitrogen cycle, excess ammonia is harmful to plants and reduces air and water quality.
- In the troposphere –where all weather takes place and where people live – ammonia gas reacts with nitric and sulfuric acids to form nitrate-containing particles.
- Those particles contribute to aerosol pollution that is damaging to human health.
- Ammonia gas can also fall back to Earth and enter lakes, streams, and oceans, where it contributes to harmful algal blooms and “dead zones” with dangerously low oxygen levels.
Lead (Pb)
- Lead is a naturally occurring toxic metal found in the Earth’s crust. But in increased quantities, exposure to it becomes extremely dangerous to health.
- Important sources of environmental contamination come from mining, smelting, manufacturing and even recycling activities.
- Young children are particularly vulnerable to lead poisoning because they absorb four to five times as much ingested lead as adults from a given source.
- Children who survive severe lead poisoning may be left with permanent intellectual disability and behavioral disorders.
Carbon Monoxide (CO)
- A toxic, colorless, and odorless gas, it is given off when fuel containing carbon, such as wood, coal, and petrol, is burned.
- If CO levels are high enough, a person may become unconscious and die. Long-term exposure has been linked with an increased risk of heart disease.
Delhi Air Pollution: Causes, Impact & Measures (The Hindu)

- 04 Nov 2023
Why is it in the News?
The air quality in Delhi-NCR declined over the past week due to a gradual drop in temperatures, calm winds that trap pollution, and a surge in post-harvest paddy straw burning across Punjab and Haryana.
Context:
- The air quality in Delhi has plummeted to hit the ‘severe’ category for the first time this season, with the AQI breaching the 450 mark according to the Central Pollution Control Board (CPCB).
- The State government implemented restrictions, including banning construction and demolition activities.
- Over the last few years, Delhi and its surrounding areas have been subject to hazardous smog, which conincides with the winter months rolling in.
- Smoke from farmers burning crop stubble, vehicle exhaust and factory emissions combine every winter to blanket the region in a toxic haze.
What is Pollution?
- Pollution refers to the contamination of the earth's environment with materials that interfere with human health, quality of life or the natural functioning of the ecosystems.
- The major forms of pollution include water pollution, air pollution, noise pollution and soil contamination.
- Other less-recognised forms include thermal pollution and radioactive hazards.
What are the Reasons behind Rising Air Pollution in Delhi?
- Delhi is one of the most polluted capital cities in the world for a variety of factors, including location (landlocked city), traffic patterns, dust, and farm fires.
- However, weather also has a significant impact.
- Typically, Delhi experiences deteriorating air quality from October to November, with improvements occurring from March to April.
- Unlike the winter season, the current weather conditions are not unfavorable.
- During winter, cool and calm weather tends to trap and intensify daily pollution, especially in northern India within the Indo-Gangetic Plain.
- In addition to local emissions, the decline in air quality is primarily attributed to an increase in fire incidents, largely resulting from the burning of wheat crop stubble in northern India especially Punjab and Haryana.
- Air Pollution in Delhi-NCR and the Indo-Gangetic Plains is a complex issue influenced by a variety of factors.
- Location: Delhi is a landlocked city compared to Mumbai and Kolkata so the level of pollution is more as the level of particulate matter and pollutants is not able to get discharged into the surrounding areas.
- Wind Direction: In October, the monsoons withdraw from Northwest India, bringing northwesterly winds.
- During summers, northwesterly winds transport dust from northern Pakistan and Afghanistan.
- Reduced Wind Speed: Winters see lower wind speeds compared to summers, making the region more susceptible to pollution.
- Delhi's landlocked position doesn't benefit from the sea breeze that disperses pollutants in other parts of the country.
- Stubble Burning: Burning crop stubble in states like Punjab, Rajasthan, and Haryana adds to the winter smog.
- This practice releases harmful gases like methane, carbon monoxide, volatile organic compounds, and carcinogenic polycyclic aromatic hydrocarbons.
- Vehicular Pollution: Vehicular emissions significantly contribute to declining air quality in Delhi during winter, accounting for about 20% of the problem.
- Dust Storms: Dust storms from Gulf countries worsen the existing pollution levels.
- Dry and cold weather results in dusty conditions from October to June, contributing to PM10 and PM2.5 pollutants.
- Temperature Drop: Lower temperatures reduce the inversion height, concentrating pollutants in the lower atmosphere.
- The inversion height is the layer beyond which pollutants cannot disperse upward.
- Firecrackers: Despite bans on firecracker sales, Diwali celebrations with fireworks contribute to air pollution.
- Construction Activities and Open Waste Burning: Large-scale construction projects in Delhi-NCR increase dust and pollution.
- Landfill sites and open waste burning also add to air pollution concerns.
Impact of Air Pollution on health:
- Respiratory Issues: Air pollution is a major cause of respiratory problems, including asthma, bronchitis, and lung infections.
- It can exacerbate existing conditions and increase the risk of developing them.
- Cardiovascular Diseases: Poor air quality is linked to heart problems, including heart attacks and stroke, as it can lead to the buildup of plaque in blood vessels and raise blood pressure.
- Cancer Risk: Long-term exposure to certain air pollutants is associated with an increased risk of lung and other types of cancer.
- Neurological Effects: Emerging research suggests that air pollution may have adverse effects on the central nervous system and could be linked to cognitive decline and mental health issues.
- Reduced Life Expectancy: Prolonged exposure to air pollution is associated with a shortened life expectancy, as it contributes to a range of health problems that can be life-threatening.
Impact of Air Pollution on Economic Growth:
- Healthcare Costs: Air pollution increases medical expenses due to illnesses, reducing economic growth.
- Lower Productivity: Poor air quality impairs worker productivity, hampering economic output.
- Tourism and Investment: Severe pollution deters tourists and investors, affecting local economies.
- Agricultural Losses: Air pollution harms crops, impacting food production and livelihoods.
- Environmental Cleanup Costs: Funds spent on pollution control divert resources from productive sectors, hindering economic growth.
What Steps Should Be Taken to Address Pollution in Delhi?
- Congestion Charge: Introducing a congestion charge for private vehicles during peak hours can alleviate traffic congestion and promote public transport or carpooling.
- Revenue generated from this charge can support green projects or subsidize electric vehicles, encouraging eco-friendly choices.
- Cap-and-Trade for Industrial Emissions: Implementing a cap-and-trade system sets emission limits for industries, fostering a market-driven approach to pollution reduction.
- This incentivizes industries to lower emissions and invest in cleaner technologies, ultimately reducing pollution.
- Drones for Pollution Control: Utilizing drones to detect and mitigate pollution hotspots is a proactive measure for managing air quality.
- Drones provide real-time air quality data with high resolution, allowing for public accessibility and targeted intervention.
- Vertical Gardens: Incorporating vertical gardens in urban areas enhances aesthetics and air quality.
- They absorb carbon dioxide, release oxygen, and create habitats for wildlife, contributing to urban biodiversity.
- Rewards for Low-Carbon Lifestyles: Promoting low-carbon living through a rewards system, such as points, vouchers, or tax benefits for eco-friendly choices like public transport or carpooling, encourages environmentally conscious behavior, reducing carbon footprints.
Government Measures to Combat Pollution in Delhi:
- National Clean Air Programme (NCAP): Aims to reduce PM10 and PM2.5 particles by at least 20% by 2024 compared to 2017 levels.
- Graded Response Action Plan (GRAP): As per a Supreme Court order, GRAP outlines actions based on different Air Quality Index categories, addressing air quality in Delhi and the National Capital Region.
- Stubble Burning Mitigation: Various short-term solutions, both in-situ and ex-situ, have been introduced to address crop stubble burning, such as Subsidy to farmers for Turbo happy seeders and bio-decomposers.
- Turbo Happy Seeder (THS) is a machine mounted on a tractor that cuts and uproots the stubble, in order to reduce stubble burning.
- Mobile Enforcement Teams: Enforce regulations against vehicular pollution, complemented by public awareness campaigns and investments in mass rapid transport systems. Phasing out old commercial vehicles is also underway.
- Cleaner Transport: The introduction of BS-VI vehicles, push for electric vehicles (EVs), Odd-Even as an emergency measure and construction of the Eastern and Western Peripheral Expressways to reduce vehicular pollution.
- Improved Farming Practices: Encouraging better disposal of crop residue and exploring cost-effective solutions, like chemical decomposition by the Indian Agricultural Research Institute, are essential for tackling stubble burning.
- "Green War Room": This initiative uses satellite data to identify sources of smog, particularly farm fires in Punjab and Haryana, and takes necessary action.
In response to a growing environmental and health crisis, antipollution measures are being strengthened. However, to ensure success, government bodies at various levels must need to gather the political will to boost investment, foster cross-boundary cooperation, and motivate both citizens and businesses to make their contributions.
India and the Asian Development Bank to establish a climate change and health hub in Delhi (The Hindu)

- 28 Aug 2023
Why in the News?
India's G-20 document states that the climate change and health hub will facilitate knowledge sharing, partnerships, and innovations to assist developing countries, while health systems will face challenges from infectious diseases and natural disasters driven by climate change.
Why in the news?
- India, in collaboration with the Asian Development Bank (ADB), is gearing up to inaugurate a climate change and health hub in the national capital.
- This initiative follows India's earlier achievement in hosting the inaugural WHO Centre for Global Traditional Medicine, located in Jamnagar, Gujarat.
- The forthcoming hub's mission is to foster knowledge exchange, cultivate partnerships, drive innovations, and extend support to nations beyond the G-20, with a special focus on developing countries.
The Significance of the Climate Change and Health Hub:
- Fostering Collaboration: This center holds paramount significance as it brings together diverse partners to engage in vital discussions regarding the far-reaching impacts of climate change.
- It provides a unique platform for shared learning and collaboration among stakeholders.
- Addressing Health Emergencies: India's recent G-20 outcome document highlights that climate change remains a key driver of health emergencies, including the resurgence of infectious diseases.
- Moreover, it exacerbates the frequency and severity of natural disasters, posing a significant threat to the capability of health systems to provide essential services.
- Boosting Resilience: Given this backdrop, it is imperative to bolster the resilience of health systems against the adverse effects of climate change.
- The G-20 outcome document outlines a commitment to prioritize the development of climate-resilient health systems, establish sustainable and eco-friendly healthcare supply chains, mobilize resources for resilient, low-carbon health systems, and promote collaboration through initiatives like the WHO-led Alliance for Transformative Action on Climate and Health (ATACH).
- Tackling Zoonotic Spillovers: The recent G-20 Health Ministers' meeting expressed concern about the rising incidence of zoonotic spillovers, leading to the emergence of new diseases.
- In this context, there is an urgent need to identify both new and existing drivers using a scientific and risk-based approach while reinforcing existing infectious disease surveillance systems.
- Global Impact: Situated in New Delhi, the Climate Change and Health Hub is poised to address these pressing issues on a global scale, serving as a hub for international collaboration and solutions.
About Asian Development Bank (ADB):
- Founded in 1966, the Asian Development Bank (ADB) is a multilateral institution that counts 68 members among its ownership, with 49 hailing from the Asian and Pacific region.
- ADB is unwavering in its commitment to fostering a prosperous, inclusive, resilient, and sustainable future for Asia and the Pacific, all while maintaining its steadfast resolve to eliminate extreme poverty.
- To achieve its noble objectives, ADB extends its support to member nations and partners through a comprehensive suite of financial instruments.
- This includes loans, technical assistance, grants, and equity investments, all aimed at catalyzing social and economic development across the region.
- In essence, ADB stands as a stalwart advocate for advancing social and economic development in Asia and the Pacific.
- As of December 31, 2019, ADB's five largest shareholders are Japan and the United States, each possessing 15.6% of total shares, followed by the People's Republic of China (6.4%), India (6.3%), and Australia (5.8%). The institution's headquarters are situated in Manila, Philippines.
About WHO Global Centre for Traditional Medicine (GCTM):
- The WHO Global Centre for Traditional Medicine (GCTM) is a pioneering knowledge hub dedicated to traditional medicine, recognized as the world's premier center of its kind.
- Situated in Jamnagar, Gujarat, it represents a remarkable collaboration between nations.
- India, as the primary investor in GCTM, has committed an approximate sum of US$ 250 million to facilitate the center's establishment, infrastructure development, and operational activities.
The GCTM is designed to achieve five key objectives:
- Archiving Traditional Wisdom: GCTM seeks to harness technology to construct a comprehensive database of traditional knowledge systems.
- Setting International Standards: It aspires to establish global standards for the testing and certification of traditional medicines, enhancing confidence in these age-old remedies.
- Global Knowledge Exchange: The center aims to serve as a global platform where experts in traditional medicine converge to share their experiences and expertise.
- Funding Research: GCTM endeavors to mobilize resources and funding for research in the field of traditional medicines, fostering innovation and scientific exploration.
- Holistic Healing Protocols: The center is dedicated to developing holistic treatment protocols for specific diseases, enabling patients to benefit from the complementary strengths of both traditional and modern medicine approaches.