Base Editing Breakthrough
- 29 May 2025
In News:
In a landmark medical feat, a nine-month-old American boy, Kyle “KJ” Muldoon Jr., became the first known human to be successfully treated using base editing, a next-generation gene editing technique derived from CRISPR-Cas9. KJ was born with Carbamoyl Phosphate Synthetase I (CPS1) deficiency, a rare genetic disorder that disrupts nitrogen breakdown, leading to toxic ammonia buildup—known as hyperammonemia—which can be fatal if untreated.
From CRISPR-Cas9 to Base Editing: Evolution of Gene Editing Tools
CRISPR-Cas9, developed in 2012 by Jennifer Doudna and Emmanuelle Charpentier, revolutionized biotechnology and earned them the 2020 Nobel Prize in Chemistry. Modeled after a microbial immune system, CRISPR works by creating “genetic memory”—capturing viral DNA and guiding the Cas9 enzyme, which acts as molecular scissors, to target and cut specific DNA sequences. This enables scientists to eliminate or repair faulty genes by inducing a double-strand break followed by insertion of a corrected DNA sequence.
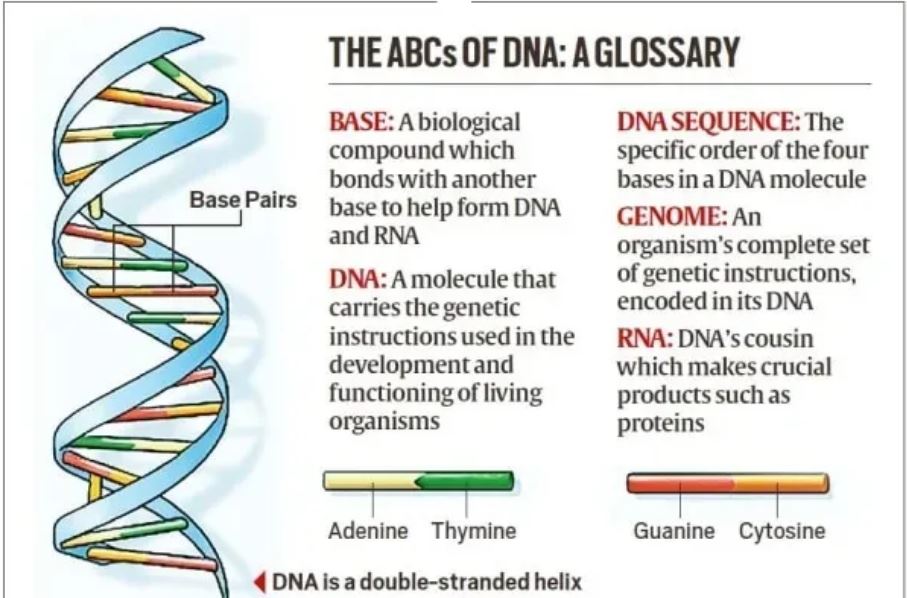
However, the double-strand break mechanism raised concerns about unintended genetic consequences. Enter base editing, a refined tool that modifies single DNA bases—the letters A, T, C, G—without cutting both strands of the DNA. Instead of scissors and glue, base editing works like a pencil and eraser, replacing one incorrect base pair with the correct one using a fusion of Cas9 and a base-modifying enzyme. In KJ’s case, the specific base mispair causing CPS1 deficiency was successfully corrected using this technique.
Advantages of Base Editing
- Precision and Safety: Avoids double-strand breaks, reducing off-target effects.
- Compactness: Easier to deliver to cells via viral vectors.
- No foreign DNA: Eliminates need for donor DNA insertion.
- Customisation: Suitable for diseases caused by single-nucleotide mutations.
Challenges: Economic, Ethical, and Regulatory
Despite its promise, base editing faces several bottlenecks:
- Cost and Accessibility: The procedure is prohibitively expensive—estimated in the range of hundreds of thousands of dollars—and was funded by research institutions and biotech firms in KJ’s case.
- Scalability: The therapy was custom-designed for KJ’s specific mutation, limiting its use for others. Such personalised medicine lacks the economies of scale that attract pharmaceutical investment.
- Regulatory hurdles: Countries like India face issues of bureaucratic red tape and outdated ethical frameworks that delay the deployment of advanced genomic therapies.
- Ethical concerns: As the technology becomes more powerful, there are concerns about misuse, eugenics, and the potential editing of germline cells.
Conclusion
KJ’s treatment marks a paradigm shift in personalised medicine, highlighting the transformative potential of base editing in addressing rare and otherwise untreatable genetic disorders. However, wider application requires systemic reforms in bioethics, regulatory frameworks, and healthcare infrastructure. To ensure equitable access, future efforts must focus on cost reduction, public funding, global collaboration, and ethical oversight. If successfully scaled, base editing could revolutionise medicine for millions suffering from rare genetic diseases.